Journal of Multidisciplinary Dental Research
Volume: 4, Issue: 1, Pages: 30-33
Original Article
Lekshmi R. Suresh1, Safeena P2, Sajna K.P3
1Senior Lecturer (Pedodontics and Preventive Dentistry), Coorg Institute of Dental Sciences, Virajpet, Karnataka, India 571218
2Postgraduate Student (Pedodontics and Preventive Dentistry), Coorg Institute of Dental Sciences, Virajpet, Karnataka, India 571218
3Postgraduate Student (Pedodontics and Preventive Dentistry)Coorg Institute of Dental Sciences, Virajpet, Karnataka, India 571218
Corresponding author
Sajna K.P.
Department of Pedodontics and Preventive Dentistry,
Coorg Institute of Dental Sciences, KK campus, Maggula, Virajpet, Coorg 571218
Phone no.: 8296780070
Email: [email protected]
Received Date:26 September 2018, Accepted Date:12 October 2018, Published Date:30 October 2018
Background/Objectives: Early Childhood caries (ECC) is a public health problem and has an impact on the oral health of children. Comprehensive review of ECC reveals significant association between socioeconomic status and the caries experience. The aim of this study was to assess the association between ECC and socioeconomic status in the Coorg population.
Methods: 40 children aged between 2-6 years who are diagnosed with severe ECC were selected along with their parents. A questionnaire was given to the parents which contained the questions regarding the information of the parent's socioeconomic status (education and occupation) and behavioural practices of the children (brushing and diet practices). Based on total scores obtained from the questions and the current Kuppuswamy index they were grouped into different strata of the society.
Results: The observations from this study exhibits that there is no inverse relationship between the socioeconomic status and Severe-ECC in the Coorg population, as stated in the literature. Alternate brushing practices like chewing in Neem stick leaves and indigenous kachi ela leaves were noted in lower lower socioeconomic status.
Conclusions: Socioeconomic factors may not play important role as the risk factor in S-ECC but it can be a potential indicator of the same
Keywords: ECC, Socioeconomic status, Neem stick leaves, Kachi ela.
Early childhood caries (ECC) is a major health concern for dental professionals worldwide. ECC is defined as the presence of one or more decayed, missing or filled tooth surfaces in any primary tooth of child age 71 months or younger.1 American Association of Pediatric Dentistry (AAPD) specifies that, in children younger than 3 years of age, any sign of smooth-surface caries is indicative of severe early childhood caries (S-ECC)2. The smooth surfaces of maxillary incisors are commonly involved in initial stage of ECC. Consequences of S-ECC are the “loss” or extraction of teeth. Extraction of the teeth is justified when the clinical conditions are serious, as a result of complications.
The prevalence of ECC is between 1-1.2% in developed countries and up to 70% in developing countries. South East Asia and Africa are shown to have increased prevalence. In European countries it is estimated to be 1-32% (England, Sweden and Finland) and 56% in Eastern Europe, in Canadian population it is less than 5%. ECC has been a serious concern in certain ethnic and immigrant groups. The prevalence of ECC in developed countries like Italy and Australia is reported to be high in pre-schoolers. In Far East Asian region, ECC prevalence is reported from 36% to 85%. In Middle East, high prevalence of caries is reported from 22% to 61% among 3 years old children. ECC is the most prevalent chronic disease in United States and unmet health need among children. In India the prevalence of dental caries reported in 5 years age group was 51.9% , 44% among 8 to 48 months old children. The prevalence of dental caries in India among 3 years old children is reported 54.1%, 4 years 42.6% and 35 years 50.7%.In pre-school children the risk factors associated in their caries experience are age of the child, educational and occupational status of their parents, feeding habits and dietary practices of the child.
Socioeconomic status also plays an important role as the risk factor for the caries development and progression in children. Literature has documented an inverse relationship between socioeconomic status and incidence and prevalence of diseases. The prevalence of ECC is believed to be increasing in low socioeconomic groups due to lack of early preventive measures and availability of adequate treatment facilities.3
The present cross sectional study was conducted to understand the association between S-ECC experience in children, aged 2-6 years and the association with the socioeconomic status of their parents.
MATERIALS AND METHODS
Out of 150 children reporting to Department of Pedodontics and Preventive Dentistry, 40 children within time period of 3 months between the age group of 2-6 year old, with S-ECC were identified. Oral examination was made by the single operator using WHO criteria to diagnose caries.
The ethical clearance from the Institutional Review Board and informed consent from the parents was obtained to participate in the study.
In total, 40 children and their parents participated in the questionnaire survey. The questionnaire was designed to assess the brushing practices of the children and their socioeconomic status comprising the questions on their education level and family income.
Using Kuppuswamy socioeconomic status scale the responses were scored for the parent's education, occupation and family income. Socioeconomic status was determined by taking the total of individual score from their education, occupation and family income and grouped. The socioeconomic status observed and grouped. The socioeconomic status observed were of 4 groups: Upper middle, Lower middle, Upper lower, Lower lower.4
occupation and family income. Socioeconomic status was determined by taking the total of individual score from their education, occupation and family income and grouped. The socioeconomic status observed were of 4 groups: Upper middle, Lower middle, Upper lower, Lower lower.4
Based on the response obtained from the brushing practices, the brushing frequency and the methods were noted. Brushing frequency observed was brushing once daily, twice daily and not brushing daily. Brushing method observed was brushing using tooth paste and brush, tooth powder and alternate methods.
RESULTS
Data was analysed using the percentage scale to evaluate the percentage of different levels of socioeconomic status of the parents and different types of brushing practices observed in the children with S-ECC.
The prevalence of S-ECC in the population was 0.2267. In 40 children with S-ECC the 45% of parents were from Upper middle class, 10% from Lower middle class, 23% from Upper lower and 10% from Lower lower class.
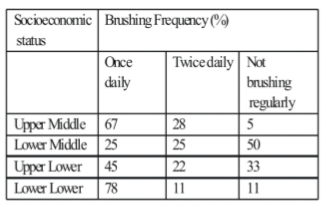
In Upper middle class 67% brushed once a day, 28% brushed twice and 5% brushed irregularly (skipped brushing for a day/two). In Lower middle class 25% brushed once and twice, 50% brushed irregularly. In Upper lower class 45% brushed once and 22% twice and 33% irregularly. In Lower lower class 78% brushed once, 11% twice and 11% irregularly
Children in lower socioeconomic groups used Neem leaves, salt, charcoal & indigenous leaves (kachi ela). This was observed to a greater extent in lower lower socioeconomic status.
Table1: Socioeconomic status and brushing frequency
DISCUSSION
Prevalence of S-ECC is reported to be high in preschoolers. ECC is identified as biological, social and behavioural effects on the children and is reported more in certain ethnic and immigrant groups. The extent of S-ECC is found different in various socioeconomic statuses.
The socio demographic factors are reported as important risk factors for caries development and progression of diseases.1 The general definition of socioeconomic status takes into account the combination of income, education and occupation/employment as these factors tend to be interrelated.4 Socioeconomic status description and assessment is challenging as it is an abstract and complete construct that presents how power and resources are distributed in society, the Kuppuswamy et al scale for the assessment of socioeconomic status is more or less comprehensive with its scoring system from the occupation, education status and income of the family.
The socioeconomic status observed were Upper middle class- 45%, Lower middle class- 10%, Upper lower class- 23% and Lower lower class-10%. This observation was not in accordance with the documentation in the literature as prevalence of ECC is continuously increasing in low socioeconomic status (SES) due to lack of early preventive measures and availability of adequate treatment facilities.
The high cost of treating ECC is considered to be significant income burden on families and this prevents from adopting appropriate preventive measure. The observations from this study demonstrated otherwise that Lower lower group brushed once daily in greater percentage and they had reduced percentage of not brushing daily. In Lower lower group they used alternate brushing practices like chewing Neem stick leaves, indigenous kachi ela leaves also salt and charcoal. Neem stick leaves and salts have proven efficacy against cariogenic bacteria.5 Charcoal in its actual form is considered to be abrasive and is not recommended for brushing. However the basic component of activate charcoal as ultra- micro charcoal particles are included in the dentifrices to benefit its anti-cariogenic property.6 This demonstrates that awareness and motivation towards oral health was high in Lower lower socioeconomic status than compared to other higher groups of socioeconomic status (Upper lower and Lower middle class). Also in Upper middle class some percentage of children did not brush their teeth on a daily basis.
The observations from this study exhibits that there is no inverse relationships between the socioeconomic status and S-ECC in the Coorg population, as stated in the literature.
In management of the ECC irrespective of the social demographic conditions of the population appropriate treatment strategies comprising customised preventive and therapeutic/restorative phase of management is recommended.
Subscribe now for latest articles, news.






















