Journal of Multidisciplinary Dental Research
DOI: 10.38138/JMDR/v5i2.1
Volume: 5, Issue: 2, Pages: 56-61
Original Article
Kathiresan Ravichandran1, Jithesh Jain2, Bhakti Jaduram Sadhu3, S.R.Ananda4, Rebecca Lilda5
1Post Graduate Student, Department of Public Health Dentistry, Coorg Institute of Dental Sciences, Virajpet, Kodagu, Karnataka, India.
2Professor and Head of the Department, Department of Public Health Dentistry, Coorg Institute of Dental Sciences, Virajpet, Kodagu, Karnataka, India.
3Associate Professor, Department of Public Health Dentistry, Coorg Institute of Dental Sciences, Virajpet, Kodagu, Karnataka, India.
4Professor, Department of Public Health Dentistry, Coorg Institute of Dental Sciences, Virajpet, Kodagu, Karnataka, India.
5Post Graduate Student, Department of Prosthodontics & Implantology, Coorg Institute of Dental Sciences, Virajpet, Kodagu, Karnataka, India.
Corresponding Author:
Dr.Kathiresan Ravichandran,
Post Graduate Student, Department of Public Health Dentistry,
Coorg Institute of Dental Sciences, Virajpet, Kodagu, Karnataka 571218, India.
Phone Number - +91 8838891967
E-mail ID : [email protected]
Received Date:23 November 2019, Accepted Date:31 December 2019, Published Date:31 December 2019
Background: Xylitol, a naturally occurring five-carbon sugar polyol, is a white crystalline carbohydrate known since a century ago. Xylitol promotes the remineralisation both by the increasing of saliva rate and inhibition of bacteria growth.
Objective: To assess the efficacy of xylitol toothpaste and chewing gum on salivary parameters - salivary pH, RFR and SFR among patients with medium cariogenic risk.
Methods: The study population comprises of 40 subjects with medium cariogenic risk were divided into 2 groups of 20 individuals each. Subjects in Group I, Group II were given xylitol tooth paste, and xylitol chewing gum for 3 weeks. The following parameters were assessed before and after the use of xylitol-based products - RFR, SFR, and salivary pH.
Results: Both groups showed an increase in the RFR, SFR and pH after three weeks. RFR was found to be statistically significant in Group I (p=0.004), Group II (p=0.000). SFR was found to be statistically significant in Group II (p=0.000). pH was found to be statistically significant in Group I (p=0.001) and Group III (p=0.000).
Conclusion: Chewing-gum is comparatively more effective than toothpaste. Considering convenience and affordability for the subjects, chewing-gum may not always be preferred and in that case mouthwash or toothpaste can be used for the promotion of better oral health.
Keywords: Chewing gum, Salivary flow, Toothpaste, Xylitol.
Dental caries is one of the most common preventable diseases which is recognized as the primary cause of oral pain and tooth loss. It is a major public health oral disease which hinders the achievement and maintenance of oral health in all age groups . WHO claimed that poor oral health may have a profound effect on general health as well as quality of life, and several oral diseases are related to chronic diseases1.
Dental caries refers to the localised destruction of susceptible dental hard tissues by acidic by-products from the bacterial fermentation of dietary carbohydrates . It is a chronic disease that progresses slowly in most of the people which results from an ecological imbalance in the equilibrium between tooth minerals and oral biofilms. Sucrose is a major environmental contributor to dental caries because many oral streptococci possess extracellular enzyme capable of cleaving the a-1 and a-2 glycosidic bond of sucrose and harnessing the energy to yield glucose polymer (glucans and mutans) and fructose. This group of enzymes called the glucosyl-transferases (GTFs), accounts for this special relationship between sucrose and caries2 .
Saliva is one of the intraoral host factors that influence caries development. Saliva is the complex mixture of fluids that surrounds the oral tissues, and it originates from major and minor salivary glands and non glandular sources such as crevicular fluids, oral microorganisms and host cells. The normal resting salivary flow rate ranges from 0.25 to 0.35 milliliter per minute. The stimulated saliva represents 80 to 90 percent of daily salivary production, and the stimulated flow rate varies from 1 to 3 ml/minute. The salivary pH and the salivary buffering capacity are determined by the hydrogen bicarbonate balance in saliva. Among the various protective functions of saliva, including diluting and cleaning the oral cavity, serving as a host defense, and buffering and enabling ion exchange, certain salivary characteristics outside the normal range of values may contribute to the caries process. Dental caries results from the dissolution of minerals from the tooth surface by organic acids formed from the bacterial fermentation of sugars. The capacity of saliva to flush microorganisms and substrates and maintain oral cleanliness may be influenced by its consistency and flow rate. Salivary pH can contribute to the ion exchanges during remineralization and demineralization of enamel, with super saturation of calcium and phosphate at pH 7 and in the presence of fluoride3.
Many things over the years have improved the way dental hygiene care is provided. Children who are caries free initially, but by adulthood, nearly 100 % have experienced dental disease. If we look closely, traditional prevention which includes brushing, flossing and fluoride toothpaste isn’t working very well . This is where xylitol is a biggest game changer than all the other improvements. Xylitol promotes the remineralisation both by the increasing of saliva rate and inhibition of bacteria growth4.
Xylitol, a naturally occurring five-carbon sugar polyol, is a white crystalline carbohydrate known since a century ago. It has been widely studied during the last 40 years for its effect on dental caries7. It is found naturally in fruit, vegetables, and berries and is artificially manufactured from xylanrich plant materials such as birch and beechwood. Since a study conducted in Turku, Finland, evaluating the effectiveness of xylitol on dental plaque reduction in 1970, xylitol has been widely researched and globally accepted as a natural sweetener approved by the US Food and Drug Administration (FDA) and the American Academy of Pediatric Dentistry 5.
Currently, more than 35 countries have approved the use of xylitol in foods, pharmaceuticals, and oral health products, principally in chewing gums, toothpastes, syrups, and confectioneries8. Xylitol is found in various products as follows: chewing gums, toothpastes, mouthwashes, breathmints and lozenges. Researches related to xylitol effects show different effects on the decreasing of dental caries incidence and changes of Streptococcus mutans levels to children, following a consume from 4 grams to 15 grams daily, divided in 3-7 doses. Xylitol decreases the incidence of dental caries by increasing salivary flow and pH and reducing the number of cariogenic (MS) and periodontopathic (Helicobacter pylori) bacteria, plaque levels, xerostomia, gingival inflammation, and erosion of teeth5.
Hence, this study was conducted to compare the efficacy between xylitol Tooth paste, and xylitol chewing gums on salivary parameters like salivary pH, saliva resting flow rate (RFR) and saliva stimulated flow rate (SFR).
To compare the efficacy between xylitol tooth paste and chewing gum on salivary parameters - salivary pH, saliva resting flow rate (RFR) and saliva stimulated flow rate (SFR) among patients with medium cariogenic risk.
The present study is a Clinical in-vivo study conducted on subjects visiting dental college between the age group of 18 – 25 years during the month January – March 2019. The study comprised of forty participants and the sampling method is based on Convenience sampling. Subjects who were willing to participate in the study and subjects with medium cariogenic risk were included in the study whereas subjects with history of antibiotics usage 3 months prior to the study, subjects under antibiotics regimen, undergoing orthodontic treatment or with extensive intraoral prosthesis were excluded from the study. The Ethical clearance was obtained from the Institutional Review Board. Written Informed consent was taken from all the study subjects who participated in the study. The subjects who participated in the study were divided into 2 groups of 20 individuals each: Group I: were given xylitol tooth paste and instructed to brush 2 times daily for 3 weeks (Figure 2).

Fig 1 - Digital pH Meter
Group II: were given xylitol chewing gums and were instructed to chew 2 pieces, 3 times daily for 3 weeks (Figure 3).

Fig 2 – Xylitol Tooth Paste
The following salivary parameters were assessed prior to the usage of xylitol products and after 3 weeks usage of xylitol-based products:
The resting salivary flow rate was measured by asking the patients to rinse their mouth with water and to rest for 1 minute. After swallowing their saliva they were asked to wait 40 seconds without swallowing and then to spit the saliva at each 2 minutes in a graded tube for 5 minutes.
The stimulated salivary flow rate was measured by asking the patients to rinse their mouth with water and then to rest for 1 min. After swallowing their saliva they were given 5 ml of lemon juice, and were asked to spit the saliva at each 2 minutes in a graded tube for 5 minutes.
Salivary pH was recorded by using digital saliva pH meter (Figure 1).

Fig 3 – Xylitol Chewing Gum
Descriptive statistics were prepared using Microsoft excel 2007 version. The data obtained was coded and fed into the SPSS (Statistical Package for Social Sciences) version 17 for analysis. Categorical data were presented as number and percentages by using contingency tables and continuous data as mean and standard deviation. Data was analyzed using Chi-square test. One way analysis of variance was used to compare the efficacy of xylitol based oral hygiene products between each groups. All statistical tests were performed at 95% confidence interval. A p value less than 0.05 was considered as statistically significant.
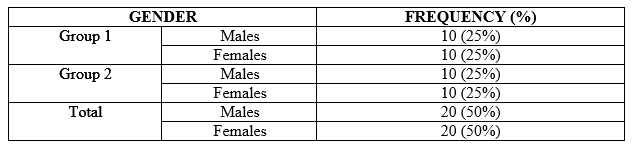
Forty subjects with mean age of 21.23 and those who had medium cariogenic risk were recruited in the present study. They comprised of 20 males and 20 females (Table 1) in which 10 males and 10 females were distributed in Group 1, whereas 10 males and 10 females were distributed in Group 2.
Table 1 - Distribution of study subjects based on gender
Comparison of salivary parameters before and after the use of xylitol tooth paste
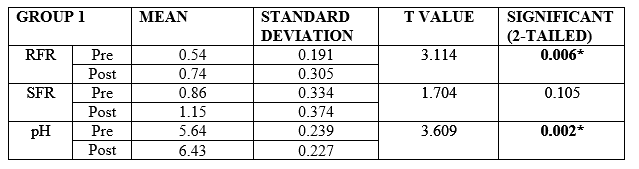
The mean RFR before and after the use of xylitol toothpaste were found to be 0.54 ml and 0.74 ml respectively. The mean SFR before and after the use of xylitol toothpaste were found to be 0.86 ml and 1.15 ml respectively. The mean pH before and after the use of xylitol toothpaste were found to be 5.64 and 6.43 respectively.
Comparison of salivary parameters before and after the use of xylitol toothpaste for 3 weeks showed that RFR (p = 0.004) and pH (p = 0.001) were found to be statistically significant; whereas SFR (p = 0.114) was found to be statistically nonsignificant (TABLE 2).
Table 2 - Comparison of salivary parameters before and after the use of xylitol tooth paste
Comparison of salivary parameters before and after the use of xylitol chewing gum
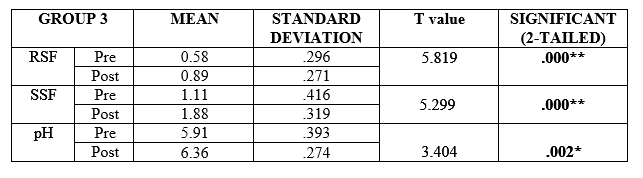
The mean RFR before and after the use of xylitol chewing gum were found to be 0.58 ml and 0.89 ml respectively. The mean SFR before and after the use of xylitol chewing gum were found to be 1.11 ml and 1.88 ml respectively. The mean pH before and after the use of xylitol chewing gum were found to be 5.91 and 6.36 respectively.
Comparison of salivary parameters before and after the use of xylitol toothpaste and xylitol chewing gum for 3 weeks showed that RFR (p = 0.000) and SFR (p = 0.000) were found to be statistically highly significant; whereas pH (p = 0.002) was found to be statistically significant (TABLE 3)
Table 3 – Comparison of salivary parameters before and after the use of xylitol chewing gum
Because of the high worldwide prevalence of dental caries and its immense health burden, there have been many interventions aimed at its prevention. Xylitol, like any other sweetener, promotes mineralization by increasing the salivary flow when used as chewing gum or large xylitol pastille. The uniqueness of xylitol is that it is practically non fermentable by oral bacteria.6 In the present study, both male - 20(50%) and female – 20(50%) participants were equally distributed and the mean age of the participants is 21.23. The findings are in accordance with the study conducted by M. Ribelles Llop et al7 in Spain wherein there was a equal gender distribution.
In the present study, it was found that the Mean Resting Salivary Flow rate, Stimulated salivary flow rate and salivary pH levels increased after the use of xylitol tooth paste (Group I). The mean resting salivary flow rate increased from 0.54 ml to 0.74, whereas the stimulated salivary flow rate increased from0.86 ml to 1.15. The results are in accordance with study by Galina Pancu et al8 in Romania, wherein the Mean Resting Salivary Flow rate increased from 0.5 ml to 1.15 ml, the stimulated salivary flow increased from 0.85 ml to 1.17 ml. In the present study, the salivary pH level increased from 5.64 to 6.43 and this result is in accordance with study by Surdacka A et al4 in Poland, wherein the pH level increased from 6.48 to 6.73.
In the present study, it was found that Mean Resting Salivary Flow rate, Stimulated salivary flow rate and salivary pH levels increased after the use of xylitol chewing gum (Group II). The mean resting salivary flow rate increased from 0.58 ml to 0.89 ml, whereas the mean stimulated salivary flow rate increased from 1.11 ml to 1.88 ml and the pH increased from 5.91 to 6.36. The results are in accordance with study by Cristina Nuca et al9 in Romania, wherein the resting salivary flow rate increased from 0.88 ml to 1.15 ml, the stimulated salivary flow rate increased from 1.20 ml to 1.66 ml and the pH level increased from 6.99 to 7.65.
In the present study, it was found that subjects who used xylitol chewing gum showed better results, wherein RFR (p=0.000), SFR (p=0.000) and pH (p=0.002) values were found to be statistically significant when compared to the subjects who used xylitol tooth paste, wherein only RFR (p=0.004) and pH (p=0.001) values were found to be statistically significant and SFR (p=0.114) was found to be statistically nonsignificant. The results are in accordance with Studies carried out by Soderling et al10 in Finland, Isokangas et al11 in Finland and Makinen et al12 in France, wherein they have shown that chewing a xylitol-sweetened chewing gum increases the salivary flow rate thereby reduces the levels of S. mutans in saliva. The results are in contrast with study by M. Ribelles Llop et al7 in Spain, where they have stated that no statistically significant differences were observed between salivary flow rate in baseline conditions and after chewing xylitol-sweetened chewing gums.
According to the review by Honkala et al13 chewing gum containing xylitol produces the best results in terms of the salivary parameters such as salivary flow, pH and low Mutans streptococcus counts in saliva. They attribute these effects to the chemical properties of xylitol. Whereas Tanzer et al,14 Soderling et al10, Alanen et al15 in their review find that chewing is essential and state that these effects are due more to the act of chewing than to the chemical composition of xylitol.
Oral hygiene products containing noncariogenic sweeteners causes the pH to rise after eating carbohydrates due to the stimulation of salivary flow, with a resulting increase in bicarbonate levels as reported by Scheinin et al16. This greatest caries reduction was due to antibacterial effect of xylitol. Tuncer et al17 in Sao Paulo stated that xylitol sweetened chewing gum had an important anti-caries effect due to the antibacterial properties of this type of sweetener, which produces a greater reduction in lactic acid. In most studies, however, this antibacterial effect is found only when chewing xylitol-sweetened chewing gum is analysed over a longer period of time.
Even in a short period of time (21 days), which is the limitation of this study, these xylitol based oral hygiene products proved to be effective as observed in the results achieved. Although the results of the present study are promising, a longer followup evaluation is required for this type of preventive procedure in high risk caries subjects who are at the initial stage of caries development.
Despite the literature data related to xylitol, new researches are needed to determine the efficacy of xylitol on salivary parameters, its optimal dosage and the daily frequency supply for an effective action against cariogenic bacteria as well as the administration ways and its adverse effects.
Xylitol is a well known anti-caries agent and it has been well documented in the prevention of caries. The present study was conducted in the light of these facts to compare the efficacy of two different xylitol products and it concludes that xylitol chewing-gum is comparatively more effective than xylitol toothpaste. Considering convenience and affordability for the subjects, chewing-gum may not always be preferred and in that case toothpaste can be used for the promotion of better oral health.
Subscribe now for latest articles, news.






















