Journal of Multidisciplinary Dental Research
Volume: 4, Issue: 2, Pages: 37-45
Original Article
Wan Nurul Izzati binti W Abd Hamid1, Nik Nur Syahiran binti Abdullah1, Annapurny Venkiteswaran1, Rohaida Abdul Halim1, Noren Nor Hasmun1
1Faculty of Dentistry, Universiti Teknologi MARA, Selangor, Malaysia
Corresponding
Annapurny Venkiteswaran
Centre of Studies in Paediatric Dentistry and Orthodontics
Faculty of Dentistry, Universiti Teknologi MARA (UiTM), Sungai Buloh Campus
47000 Sungai Buloh, Selangor, Malaysia
Phone:(+603) 6126 6445 / 6633
E-mail: [email protected]
Received Date:11 October 2018, Accepted Date:16 October 2018, Published Date:25 October 2018
OBJECTIVES: To compare the preferences of patients and clinicians perception towards two different methods of audiovisual distraction in behavior management approach.
MATERIAL AND METHODS: A total of 21 children were included in this study. The children were assessed over two visits during which they were given different types of audiovisual distraction which were a cartoon show and an interactive game. Children's pre-operative anxiety level was assessed using the Facial Image Scale (FIS). The pulse rate of the patients was taken using pulse oximeter during 5 stages of dental treatment on a patient. A post-op modified MCDAS questionnaire was given to the patient to measure the patient-perceived pain level. A self-administered questionnaire was also given to the operator after the treatment to assess the operator's perception in using audiovisual distraction in managing paediatric patients.
RESULTS: There were no statistically significant differences in heart rate between cartoon and interactive games, but it was noted that there was a significant increase in the heart rate during administration of local anaesthesia, followed by placement of clamp. Besides that, there were significantly different in MCDAS scoring between cartoon and games, which showed patients with cartoon, had lowered score compared to interactive games. (p<0.05)
CONCLUSION: Result of this study showed that both types of audiovisual distraction, interactive games and cartoon are effective in reducing anxiety among paediatric dental patients. Although there was no significant difference in heart rate, the children seemed to prefer cartoons over games. The preferred method of audiovisual distraction among clinicians was also cartoon.
Keywords: audiovisual distraction, paediatric patient, dental anxiety.
The very mention of seeing a dentist brings about anxiety in patients of all ages. So it is no surprise that dental fear and anxiety pose a greater challenge to clinicians rather than the technical aspect of a treatment itself. Dental anxiety can be defined as abnormal fear or dread of visiting the dentist for preventive care or therapy and unwarranted anxiety over dental procedures.1 During dental visit, most patients will normally experience some type of tension or fear, with some patients experiencing moderate to severe anxiety. This has been suggested as one of the main reasons why most patients avoid seeing a dentist. Pain or fear of pain is a primary source of anxiety as well as being a major obstacle to seeking dental care.2 Anxious patients usually feel more pain during injections of local anesthesia and of longer duration than less anxious patients. 3Studies also show that anxious tend to present with more oral health problems compared to less anxious and more cooperative patients.4,5 Other than that, dental anxiety also creates a significant problem to the dental professionals. There are many techniques that can be used by the dental professionals in managing anxious patients such as tell-show-do, relaxation, distraction, systematic desensitization, modeling, audio analgesia, hypnosis and behavioural rehearsal.6 The most widely use method is the tell-show-do technique. The success of technique tell-show-do is well documented, nevertheless it is not always suitable or adequate for every patient as some patients are too young to understand what the dentists are trying to convey.
Distraction is defined as a technique of diverting a patient's attention from what may be perceived as an unpleasant procedure. The objectives of distraction are to decrease the perception of unpleasantness and avert negative or avoidance behaviour.7 Distraction has been shown to be effective in pain reduction experienced in short invasive medical procedures. It is favourable as it is safe, inexpensive, and effective. 8Over the years, the use of audiovisual distraction has gained popularity in reducing anxiety in paediatric patients. This method allows the patient to use two of their senses to help further their distraction potential. Perception of pain decreases when a person's attention is distracted away from the pain stimulus.9 This can be accomplished using audiovisual distraction technique.10
Measurement of heart rate is a reliable biofeedback representation of anxiety and thus it was chosen as a tool to compare anxiety levels in this study. Other than that, Faces version of Modified Child Dental Anxiety Scale (MCDAS) Questionnaire is an effective assessment of anxiety as it is was easier for younger children to relate to pictures rather than values alone.11 This index is self-reported and consists of 8 questions with 5 pictorial answers for each question. Scores on the MCDAS scale may range from 8 to 40, with scores below 19 indicating absence of state anxiety, scores higher than 19 indicating the presence of state anxiety and scores higher than 31, indicating severe phobic disorder.12 This scale is used because it is proven that MCDAS measure has adequate reliability, validity, sensitivity and specificity.[13] Besides that, a self-administered questionnaire was given to the operator after the treatment to assess the operator's perception in using distraction in managing paediatric patients.
To date, there are many studies that have proven that audiovisual distraction is effective in alleviating anxiety in paediatric patients. The present study was undertaken to evaluate which types of audiovisual distraction either video games or cartoons was more effective. This will help the clinician to modify the method in managing anxious dental patient and thus make it easier for the clinician to do the treatment.
MATERIALS AND METHODS
The study was approved by the Faculty of Dentistry UiTM Sungai Buloh ethics review board, University Technology of Mara. Parents of children who participated in this study signed a consent form prior to the questionnaire distribution.
A total of 21 children aged from four to eight years old who attended Department of Paediatric UiTM Sungai Buloh had participated in this study. The children who were chosen to participate in this study had met the following criteria which are healthy, has carious teeth, conscious, able to respond adequately and appropriately to questions and the patients and their parents agreed to participate in this study. The exclusion criterias consist of children who have history of cardiac problem and have history of polycythemia or anaemia, caries free, limited cooperation and any children who used rotary toothbrush at home.
The pulse oximeter used in this study was OL2700 (Nihon Kohden Oxypal®) and the machine was well calibrated throughtout its use during the study. In this study, two types of local anesthesia were used, topical local anesthetics (Topicale® – gel pump, 43g, 3/Pkg) and injectable local anesthetics (4% Articadent® Dental Articaine HCl with Epinephrine – 1.7 ml Injection Cartridges) . For topical local anesthetic, it comprises of 18% Benzocaine and it has patient- pleasing flavors while for injectable local anesthetics (Citocartin® 100 – consisting Articaine hydrochloride 4% with adrenaline 1: 100 000). Metal dental syringe (Aspiject®) and short needles were used in all the cases.
Rubber dam is used for better access and visualization and moisture control. Rubber dam placement prevents the swallowing and aspiration of foreign bodies and protection of the soft tissues. For many children placement of a rubber dam results in enhanced cooperation but in some cases, the placement of the clamp can be uncomfortable or anxiety provoking. The rubber dam acts as a barrier so that the procedures are perceived as less invasive and reduces the handpiece water spray from accumulating in the mouth.
For rotary instrument, high speed handpiece with 200,000 rpm speed was used. This handpiece is used to remove decay, remove old restoration and for polishing purposes.
Facial Image Scale (FIS) was used pre-operatively to assess child dental anxiety to the dental procedure. FIS is the most appropriate scale to use as it is more easier for the child to make a choice. Furthermore, it is easy for the clinician to distribute and administer the picture scale. Besides that, the Modified Child Dental Anxiety Scale (MCDAS) questionnaire was also used postoperatively to measure the patient-perceived pain level. This scale is used because it is proven that MCDAS measure has adequate reliability, validity , sensitivity and specificity.9
Before the treatment started, the operator explained the objectives of the study to the children as well as their parents/guardian, got their consent, and gathered the information regarding the patient's medical and dental history. The child was assessed over two visits whereby two different audiovisual distractions were used. The type of audiovisual distraction used in the first visit is different from the second visit. The type of audiovisual distraction used in the first visit was randomly selected by the operator either interactive games or cartoon movies. Facial Image Scale (FIS) was used to assess the child's anxiety level pre-operatively. The pulse rate of the patient was taken immediately when the patient sat on the dental chair as a baseline, during placement of topical anaesthesia, during injection of local anaesthesia, during placement of clamp and rubber dam, and during onset of caries removal with rotary insturment. A post-op modified MCDAS questionnaire was given to the patient to measure the patient-perceived pain level. Other than that, a self administered questionnaire was given to the operator after the treatment to assess the operator's perception in using distraction in managing paediatric patients.
The statistical analysis of the measurements was performed with statistical software (SSPS Statistics 23, IBM, Chicago, IL, USA). Kruskal Wallis test was used to evaluate the difference of Facial Image Scale (FIS) between the cartoon and games. In addition, Kruskal Wallis test was also used to evaluate the MCDAS score on effect of age and inter-gender in between cartoon and games. Wilcoxon test was used to determine the change of mean heart rate between the 5 procedures in both cartoon and game distraction. Friedman test was used to determine the ranking of anxiety based on increase of heart rate. Lastly, pie chart was used to evaluate the most preferrable audiovisual distraction technique, cartoon or games in managing anxious pediatric dental patients.
RESULTS
Data on the types of audiovisual distraction used on the participants are presented in Graph 1 and Graph 2. There is no statistically significant difference between cartoon and games. However, the children between the age of 5-to-6 were found to be happier when cartoon was used and none was recorded for games. It can be noted that the children aged 8 years preferred games of cartoon.
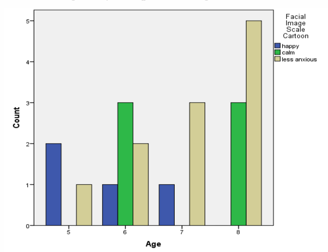
Graph 1 Children's dental anxiety level (FIS) with cartoon, by age
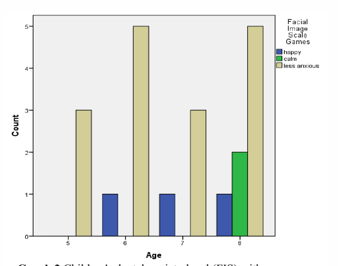
Graph 2 Children's dental anxiety level (FIS) with games
Table 1 presents the heart rate of the children at baseline, during topical anaesthesia application, local anaesthesia administration, placement of rubber dam and clamp and during caries removal. There is no statistically significant difference in heart rate between cartoon and interactive games. However, it was noted that the highest increase in the heart rate was during the administration of local anaesthesia, followed by placement of clamp, onset of caries removal and placement of topical anaesthesia. An assessment of the operator's perception towards mode of audiovisual distraction used was done and it was noted that majority of the operator preferred cartoon as the mode of audiovisual distraction (76.2%).
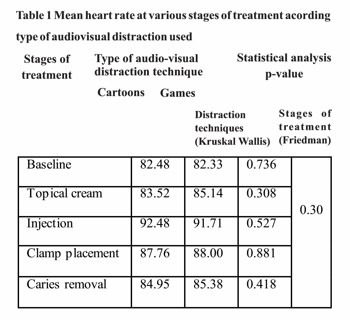
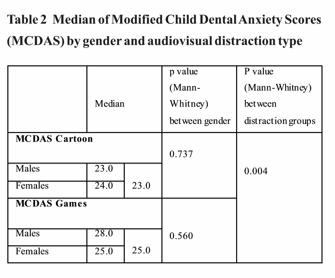
Table 2 presents the median value for post operative treatment Modified Child Dental Anxiety Scores (MCDAS) for both audiovisual distraction, cartoons and games. The median value for MCDAS scores for cartoon is 23.0 and the median value for MCDAS scores for games is 25.0. There is statistically significant difference between cartoon and games (p= 0.004). The median value of MCDAS scores for males cartoon is 23.0 and the females cartoon is 24.0. There is no statistically significant difference between males and females (p=0.737). Median value of MCDAS scores for males games is 28.0 and females games is 25.0. There is no statistically significant difference between males and females in games (p=0.560).
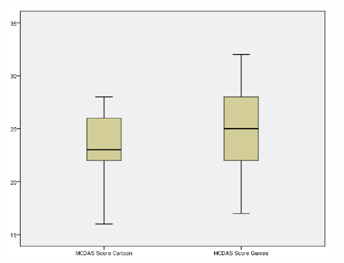
Graph 3 Boxplot of the range of MCDAS scores for cartoon and games
DISCUSSION
Dental anxiety in children poses a significant problem to the dentist. The beneficial effects of the preventive dental care are also limited due to this. Alleviating a child's anxiety about dental treatment procedure is therefore important in preventing apprehension that may later continue 14into aldulthood. The aim of this study was to compare which audiovisual distraction is effective in managing anxious peadiatric patients during restorative treatment. This study is a repeated measure in which the patients were given both audiovisual distraction, cartoon and games. Repeated measures ensures that other confounding factors did not affect the results. A crossover model was used, whereby some subjects were assigned to cartoon and the other were given interactive games for the first visit. Findings of the current study helped to determine clinician's perceptions in using this type of distraction. In the current study, we have used Facial Image Scale (FIS), Faces version of Modified Child Dental Anxiety Scale (MCDAS) questionnaire were used to measure anxiety. This is because MCDAS measures were proven to have adequate reliability, validity , sensitivity and specificity.13
Findings from the current study indicate that there is no statistically significant difference between the cartoon and games when Facial Image Scale was used before the treatment. The findings are consistent with several previous studies which found that distraction with cartoon can reduce pain or anxiety in dental patients.15 Many animated cartoon characters have become a public domain such as Upin Ipin and children are often obsessed with them. Previous studies have shown that the rising trends in cartoon aired on our local television channels , and exposure to the media at a very young age are among the main reasons why the children were found to be happier when cartoons was used.16 In this study, three popular cartoons in Malaysia were played to them for the children on the monitor. This indirectly proved that the intervention of viewing animated cartoons to reduce anxiety can be used without incresing the health care costs. Other than that, this intervention is easy to administer compared to interactive games since it only required the children to view it from the monitor. Result from the study also shows that the children's anxiety levels decline with age. This findings are in agreement with previous study that showed young children responded more adversely to dental 17care. Young children may lack the cognitive ability to sustain a concentrated and selective focus for their attention. They are also unlikely to consider their anxiety or distruptive behaviours as inapporpriate. Indeed, resisting distraction and maintaining a high level of vigilance may be appropriate adaptive behaviour for young children in an unfamiliar, ambiguos and potentially threatening setting such as dental clinic.18
For Modified Child Dental Anxiety Score (MCDAS), the result showed that the pediatric dental patients who were shown cartoon have less anxiety than patients who were given interactive games. In relation to the MCDAS, the higher the score, the more anxious the patient is. The scores on the MCDAS scale may range from 8 to 40, with scores below 19 indicating absence of state anxiety, scores higher than 19 indicating the presence of state anxiety and scores higher than 31, indicating severe phobic disorder.21 The majority of patients in this current study presented with a score ranging between 19 to 30, which indicate the presence of anxiety. The pattern of MCDAS scoring differs between the two groups, it was noted that a few subjects scored more than 31 in the interactive games group. The reason why the level of anxiety of patients are higher when given games is still unknown. There are no previous reports on the effectiveness of interactive games in comparison to cartoon as audiovisual distraction. Most of the researches done only compares between effectiveness of audio and audiovisual distraction. There were studies concluded audiovisual distraction was found to be more effective than audio distractions in management of anxious children.7, 22
The current study shows that age has an effect on the MCDAS scoring. The result was statistically significant in the interactive games group. It was noted that the children between the age of 5-to-6 were happy when cartoon was used as opposed in interactive games. From the result, eventhough the MCDAS scories varied at all ages among 4 to 8 years old, however, this showed that patients were less anxious with cartoon as audiovisual distraction compared to interactive games. This study should be continued with an increased sample size to better understand the relationship between the audiovisual technique and MCDAS scoring. In addition to that, MCDAS questionnaire was found to be valid and reliable as well as useful in the assessment of dental anxiety in a wide age range of children attending for dental care.23 This finding is similar to Rashidah et. al's study that MCDAS is versatile to be used for assessing dental anxiety over a wider age range for children from 5 to 12 years.[24] In agreement with the same study, it is found that all the children understood the meaning of the picture cards and were in agreement with each other on the rank order of the cartoon faces from very happy to very sad.24 Hence, the same method can be implemented in future studies with wide range of age and greater number of samples.
Apart from that, the findings of the current study also revealed that there were no statistically significant differences in heart rate between cartoon and interactive games. However, there was a remarkable increase of heart rate during the administration of local anaesthesia, followed by placement of clamp, onset of caries removal and placement of topical anaesthesia. The use of local anaesthesia which contains epinephrine which acts as a vaconstrictor may cause the increase of the children's heart rate during administration of local anaesthesia. There are many studies that shows epinephrine-containing local anesthesia can increase heart rate, cardiac output and peripheral vasodilation19,20.
The questionnaire about the operator's preferences was also distributed to the operator to determine the most preferrable audiovisual distraction, games or cartoon to be used in managing anxious pediatric dental patients. From the result, majority of the operator chose cartoon to be used as audiovisual distraction in managing their patients. The operator was asked personally the reason of why they preferred cartoon rather than games. It was found that they preferred cartoon because it was easier for them to handle the patient as the cartoon was played on monitor and patients just watched the cartoon from the dental chair. As monitor was attached to the dental chair, there was no interuption while treating their patients. This is in contrast to playing interactive games whereby the The operators reported that the patients tend to hold the tablet close to the oral area and this limit the operator's view of their work space . Scientifically, there was no study done yet comparing the effectiveness of cartoon and games, thus no comparison of results can be done.
Conclusion
In conclusion, there were no statistically significant differences in heart rate between cartoon and interactive games, but it was noted that there was an increase in the heart rate during the administration of local anaesthesia, followed by placement of clamp, onset of caries removal and placement of topical anaesthesia. In addition, the pediatric dental patients who were given cartoon had less anxiety than patient who were given AV games in relation to the MCDAS. Therefore, from this study it can be concluded that both audiovisual distractions, cartoon and games are effective in reducing the level of anxiety among the pediatric dental patients, but the preferred choice by both subjects and operators is cartoon
Subscribe now for latest articles, news.






















