Journal of Multidisciplinary Dental Research
Volume: 4, Issue: 1, Pages: 34-38
Case Report
Shashidara R1, Sudheendra U.S2, Aparna H.G3, Kavita A.P4
1MDS, Professor, Department of Oral Pathology, Coorg Institute of Dental Sciences, Virajpet.
2MDS, Professor, Department of Oral Pathology, Coorg Institute of Dental Sciences, Virajpet.
3MDS, Senior lecturer, Department of Oral Pathology, Coorg Institute of Dental Sciences, Virajpet.
4MDS, Reader, Department of Oral Medicine, Coorg Institute of Dental Sciences, Virajpet.
Correspondence:
Shashidara R,
Professor, Department of Oral Pathology,
Coorg Institute of Dental Sciences, Virajpet- 571218.
Phone: 08274- 256479 Fax: 08274- 260156
E-mail: [email protected]
Received Date:30 September 2018, Accepted Date:15 October 2018, Published Date:02 November 2018
Multiple Idiopathic Cervical Resorption is a rare disease of the tooth in which there is progressive cervical resorption of multiple teeth leading to exfoliation of crown. The etiology of such type of resorption is largely unknown with the histopathology often resembling granulation tissue. Treatments suggested include surgical exposure with subsequent restoration or extraction and replacement of affected teeth. We present a case report of multiple idiopathic cervical resorption in a 32 year old male patient.
Keywords: Tooth Resorption, Multiple Tooth Resorption, Cervical Resorption, Idiopathic Resorption.
Root resorption is a common finding in dental practice. The lesions are usually localized to the apex or middle third of the root and are associated with definite etiological factors.1 Root resorption can be classified by its location in relation to the tooth surface involved as internal and external. External root resorption has been reported to occur secondary to trauma, infection, periodontal disease, endodontic treatment and encroachment from neoplasms.2 External root resorption can further be classified into surface resorption, external inflammatory resorption, external replacement resorption and transient apical breakdown.3
The rarest and least understood type of external root resorption is external cervical resorption and has been described at length by Heithersay who preferred the term invasive cervical resorption to describe its aggressive behavior.3 This type of resorption usually involves a single tooth and has been attributed to various etiological factors. However, rare cases will present without any local or systemic etiological factors and involving multiple teeth, such resorption is called multiple idiopathic cervical resorption. It is described as an entity that demonstrates pathognomonic deep cervical resorption of vital teeth originating at cementoenamel junction.2
Generally lesions of multiple idiopathic cervical resorption are found serendipitously on radiographs or during routine clinical examinations when destruction of tooth structure is already advanced.4 The lesions are sometimes too extensive to treat and progress and/or recur despite intervention. Such lesions also present a restorative challenge because of their sub-gingival location creating problems in isolation. We present a report of one such case.
CASE REPORT:
A 32 year old male patient presented with a complaint of missing teeth in the upper left and right back jaw region and desired replacement for the same. He was apparently well seven months back when he noticed pain and sensitivity in the upper right back tooth region and within one and a half months all the upper back teeth were mobile. The patient then had visited a dentist who had extracted the mobile upper right back teeth and had performed root canal treatment (RCT) procedure for 25. At the time of presentation to us the patient was asymptomatic. Intra Oral Peri-Apical Radiograph taken during the treatment six months back showed retained root stumps of 27 and extensive cervical radiolucency involving pulp of 26. 25 showed a resorption localized only to the distal aspect with no changes noticed mesially.
Medical history and family history of the patient was non-contributory. A detailed clinical examination revealed clinically missing 15, 16, 17, 26 and 27. 25 was found to be grade III mobile. Oral hygiene and periodontal status were found to be satisfactory. 24 and 25 gave negative response to electric pulp vitality tests.
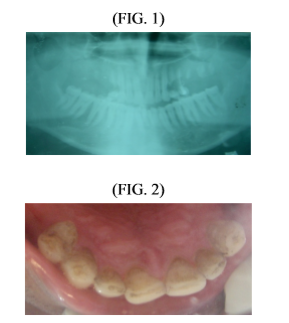
Patient was subjected to Intra Oral PeriApical Radiograph (IAPOR) in relation to 25 and orthopantomograph. IOPAR revealed radioopacity of the crown involving the pulp, root canal of 25 suggestive of endodontic treatment. Cervical radiolucency involving the pulp, crown and extending till the middle third of the root was seen with no obvious periapical changes. Extensive cervical radiolucency involving crown, root and extending to the pulp of 24, cervical radiolucency on the distal aspect of 23 and root stumps in relation to 26 region were also noted (FIGURE 2). Orthopantomograph revealed 13 and 14 showing the same pattern of cervical radiolucency. None of the involved teeth showed periapical changes. Root stumps were noted in relation to 17, 26, 27 and 28. The mandibular teeth appeared normal (FIGURE 3). The radiographic diagnosis of multiple cervical root resorption was considered.
The patient was further subjected to biochemical investigations including serum calcium, alkaline phosphatase, thyroid and parathyroid function tests. All parameters were found to be within normal range. Extraction of remaining root stumps and teeth 24, 25 with concurrent biopsy of surrounding tissue was advised. The histopathological picture was suggestive of granulation tissue.
Based upon the clinical history, clinicoradiographic and histopathological findings, a final diagnosis of Multiple Idiopathic Cervical Resorption was arrived upon.
Restoration of 13, 14 and 23 was performed with calcium hydroxide and glass ionomer cement a partial denture. The patient is on periodic followup including clinical and radiographic assessment and has not shown any progression of the lesion since the last six months.
DISCUSSION
The first case of Idiopathic Cervical Resorption was probably reported by Mueller and Rony in 1930.3 Since then a number of cases have been described. The etiology of this type of resorption however remains elusive.
Multiple Idiopathic Cervical Resorption may affect a single tooth, multiple teeth or very rarely the entire dentition. Stafne and Slocumb4 have reported that only 19 of the 179 cases of idiopathic resorption reviewed by them affected more than one tooth. Out of the 19 cases involving multiple teeth 2 teeth were involved in 17 and 3 in 2 cases respectively. Hopkins and Adams5 have reported a case of extensive idiopathic cervical resorption in a 20 year old female patient which in a three year period proceeded to involve the entire dentition. Lydiatt et al presented a case of a 39 year old female patient with multiple idiopathic cervical resorption that eventually affected all maxillary teeth biopsy of the gums revealed only a non-specific inflammation.6 Kerr et al have noticed a female predilection in their cases.7 Similar reports have also been published by Moody8 and Moody and Muir.9
Multiple Idiopathic Cervical Resorption has largely occurred in adults; however Kim et al describe a case of multiple idiopathic cervical resorption in a seven year old girl involving all deciduous teeth without any apparent etiological factor.2
George and Miller have observed the following common features in cases with Multiple Idiopathic Cervical Resorption10.
Liang H, Burkes EJ and Frederiksen NL in their systematic review have noticed that multiple idiopathic cervical resorption presents with a female predominance as an asymptomatic condition with the number of involved teeth ranging from 5 to 24. The gingival tissue surrounding the affected teeth may be healthy or chronically inflamed and the patients have a noncontributory medical history. Radiographically the lesions begin at the mesial or distal CEJ and proceed to involve the entire cervical region. The initial presentation is of a scalloped radiolucency that in time undermined enamel and extended for a variable distance down the root surface or toward pulp11. A familial pattern of multiple idiopathic cervical resorption has been reported by Neely Al and Gordon Sc12.
Several treatment modalities have been suggested in literature. Essentially treatment consists of complete removal of resorptive tissue and restoring the resultant defect with composite resin or GIC have been recommended13.
Multiple Idiopathic Cervical Resorption may occur spontaneously in the absence of either local or systemic factors or may occur due to various factors such as tetracycline root conditioning14, Guided Tissue Regeneration15,surgeries16, RCT and bleaching13.
Orthodontic treatment or trauma13 have also been proposed to cause such type of resorption, however none of the reported cases in dental literature show up with a definite etiological factor, hence prediction and prevention of such cases are very difficult. Treatment is compounded because of lack of etiological factors. Unless early treatment is initiated, the resorption progresses to a large irreversible loss of tooth structure.1
The treatment protocol that we have decided for our patient, considering available literature on Multiple Idiopathic Cervical Resorption will include, sub and supragingival curettage to remove the resorbing tissue followed by RCT for involved canine with the post and core supported over denture. The patient is currently on this treatment protocol and follow-up.
CONCLUSION
The present case involved Multiple Idiopathic Cervical Resorption of maxillary teeth with the loss of molars and premolars and involvement of canine. The present case seemed to be a true multiple idiopathic cervical resorption since none of the factors usually associated with resorption were found. All the biochemical and histological findings being negative, we reached to a diagnosis of Multiple Idiopathic Cervical Resorption. Multiple Idiopathic Cervical Resorption is a condition which is comparatively rare and difficult to manage. It is important for the clinician to realize that this lesion may not be a common endodontic problem. Treatment protocol should include maintenance of pulp vitality and proper prosthetic rehabilitation.
Subscribe now for latest articles, news.






















