Journal of Multidisciplinary Dental Research
Volume: 4, Issue: 1, Pages: 24-29
Original Article
Neveda Baskeran1, Subramanian EMG2
1Professor And Head, Department Of Pedodontics , Saveetha Dental College , Chennai , India
2Cri, Saveetha Dental College , Chennai , India
Corresponding
Neveda Baskeran , Cri ,
Saveetha Dental College , 162, Poonamalle High Road , Velappanchavadi , Chennai 600077. Email Id:- [email protected]
Received Date:26 August 2018, Accepted Date:10 October 2018, Published Date:30 October 2018
AIM:- To assess the behaviour of children with single and double hair whorls during dental treatments.
OBJECTIVE: -To compare the behaviour and cooperative ability of children with single and double hair whorls.
BACKGROUND:-Various researches have been done to assess the influence of minor anomalies on the hyperactivity of children. Minor anomalies like head size, hypertelorism, hairline , electric hair, low set ears with adherent lobes, malformed pinnas and number of hair whorls, were compared with the hyperactivity of children. As there were no evident research done comparing the number of hair whorls and behaviour of children in a dental setup, a pilot study was done . The study was done in 20 children who came to Saveetha Dental College for treatment. The number of hair whorls were correlated with behaviour of children during their subsequent dental treatments. Wright's modification of Frankl's behaviour rating scale was used to assess the behaviour .
REASON:- This helps the dentist to be prepared and plan treatment according to the number of hair whorlsof children.
OKCs are certainly among the most studied and controversial lesions in Oral pathology. The term was first used by Philipsen in 19561. The behaviour of odontogenic keratocyst (OKC), is still being debated in the scientific community. Until recently these lesions were known as Keratocystic Odontogenic Tumor (KCOT)2. Most OKC are known to arise from the cell rests of Serre. They tend to enlarge at the expense of the medullaryspace and produce clinically evident swelling only in the later stages. They can cause significant facial asymmetry and may be associated with pain, purulent discharge. On few circumstances OKC occurring in the mandible are reported to have caused altered sensation ranging from parasthesia to significant pain.
Histopathologically there is the presence of microcysts in the cystic wall which is one of the well established cause for the recurrence even 1after surgical enucleation.Besides, it has been noted that OKC are among the most prominent feature of Nevoid Basal Cell Carcinoma Syndrome (NBCCS), also known as Gorlin-Goltz syndrome.3,4 The present study was conducted to retrospectively analyze the clinical and radiographical features of OKC.
MATERIALS AND METHODS
The clinical and radiographic data, of patients attending the outpatient Department of Oral Medicine and Radiology, Coorg Institute of Dental Sciences from January 2008 to May 2017, with a histopathological diagnosis of OKC were retrospectively evaluated.
Clinical details pertaining to patient`s gender, age, site of the lesion, size(< 4 cm or >4cm), presence of multiple lesions if any, clinical features if any suggestive of Basal cell Nevus syndrome were recorded. Radiographic analysis included the location, margins, internal structure and effects on the surrounding structures.
Cases with complete clinical and radiographic data and histopathologic diagnosis of OKC according to WHO 20052 formed the inclusion criteria. Those cases with poor quality radiographs and incomplete data were excluded from the study.
RESULTS
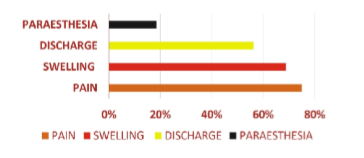
A total of 18 cases comprised the study group. The data obtained was subjected to descriptive statistics. 77.7% of the patients were (14 ) males and 22.3% (4) females.(Table 1,2). 16.6% (3) of them occurred in the first decade, 22.2% (4 cases) occurred in the second decade, 22.2% of them (4 cases) occurred in the third decade, 3 cases each (16.6%) occurred in the fourth and fifth decade respectively (Graph 1). In the present study only 1 case (5.5%) occurred in the sixth decade of life. 78% of them affected the mandible and 22% of them affected the maxilla(Table 2). Out of these 18 cases 72% (13 cases) of them had pain as the presenting symptom. (Table1,Graph 2). Swelling of the jaw bone was present in 72% (13 cases) of them (Table 1, Graph 2). Only 3 patients (16.6%) experienced parasthesia and 9 out of the 18 patients (50%) had purulent discharge from the lesions (Table1, Graph 2). Only 2 cases (11%) the lesions were multiple and these (one male and one female) patients had clinical features fulfilling the 2 major criteria for NBCCS.
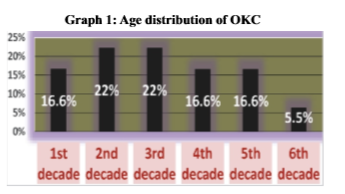
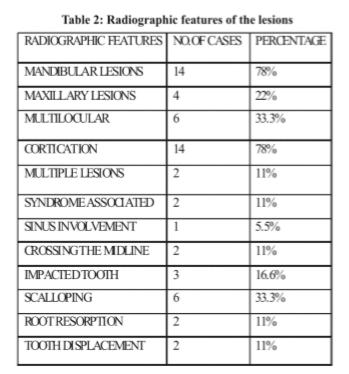
Table 1: Description of the various clinical features and radiographic features of the cases.
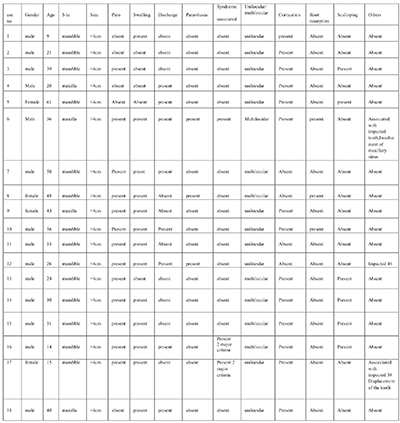
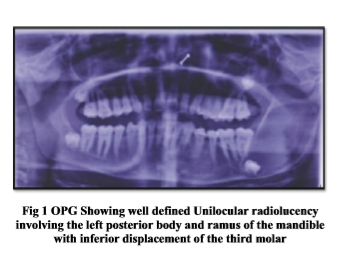
33% of the OKC in the present study were multilocular and 67% of these were unilocular (Table 2, Fig 1 OPG pic ). 78% (14 cases) of them showed corticated margins and only 33.3% showed the characteristic feature of endosteal scalloping(Table 2). In the present study only one case (5.5%) showed involvement of the maxillary sinus (Table 2, Fig 2 & 3). Out of the 18 cases only 3 cases (16.6%) the cyst was associated with an impacted tooth (Table 2). Only 2 cases (11%) showed resorption of the tooth root in the vicinity of the lesion and 2 cases (11%) showed displacement of the teeth which were associated with the lesion. In the 2 patients (11%) with NBCCS, the mandibular lesions were multiple. (Table 2).
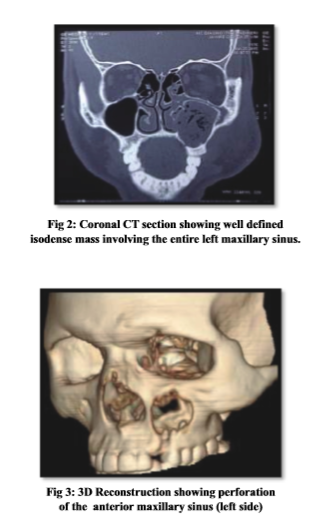
present study, patients experienced swelling, pain and purulent discharge. Two of these five patients had lesion which was associated with carious tooth in the proximity of the lesion. The rest three cases the lesion caused perforation of the alveolar bone with spontaneous discharge of cystic contents into the oral cavity and the lesion was secondarily infected.
Multiple OKC, cutaneous nevi, palmer planter pitting, rib anomalies, basal cell carcinoma are predominant characteristic features of Nevoid basal cell carcinoma syndrome.3, 4 Veenstra-Knol et al have proposed diagnostic criteria for NBCCS. Accordingly the presence of 2 major criteria or 1 major and 2 minor criteria are to be met necessary for the diagnosis of NBCCS.11 In our case series one of the patient had multiple lesions involving the mandible and maxilla and was associated with impacted teeth. The patient also had palmer plantar pitting and bifid rib. Similarly another patient had multiple lesions involving the mandible along with the presence of bifid ribs, pectus carinatum, and winged scapula. Both these patients did not have cutaneous nevi and any evidence of basal cell carcinoma. Gene testing for confirmation of mutation of PTCH gene was not done as they fulfilled the criteria for the diagnosis of NBCCS. This is in accordance with previous case reports.12,13
OKC could present as a unilocular or mutilocular radiolucency and is often well defined with corticated margins. The periphery of the lesion often shows endosteal scalloping which produces a pattern of multilocularity of the lesion. This could be due to varied growth which is multiplanar. Expansion is often minimal or absent. Displacement of teeth is often present in OKC but root resorption is rare.14 Multilocularity tends to be seen more frequent in larger lesions. According to Browne multilocularity is seen 23% and Forssel in 25%15, 16 In the present study we found only 33.3% of the lesions were multilocular and the rest 67% of them being unilocular. Presence of well-defined cortication was present in 78% cases. Endosteal scalloping was seen in 33% of the cases and root resorption was observed in only 2% of cases which is in concordance with the previous lierature16 ,17 Displacement of the tooth was present only in one case which is in contrast to the earlier case reports.15, 16, 17 In the present case series only 1 one case had involved the maxillary sinus and also had caused displacement of the inferior orbital floor. The lesion was also associated with the impacted maxillary tooth. This was in concordance with the previous literature.18,19
CONCLUSION
A retrospective analysis of a case series of OKC has been presented. The mandible was involved more frequently than the maxilla with imaging characteristics similar to the cases reported in literature. Correlation between clinical, imaging and histopathological features could shed further information regarding their behavior.
Subscribe now for latest articles, news.






















